Bottoming Out Gallery
Bottoming Out Patient 01












Description:
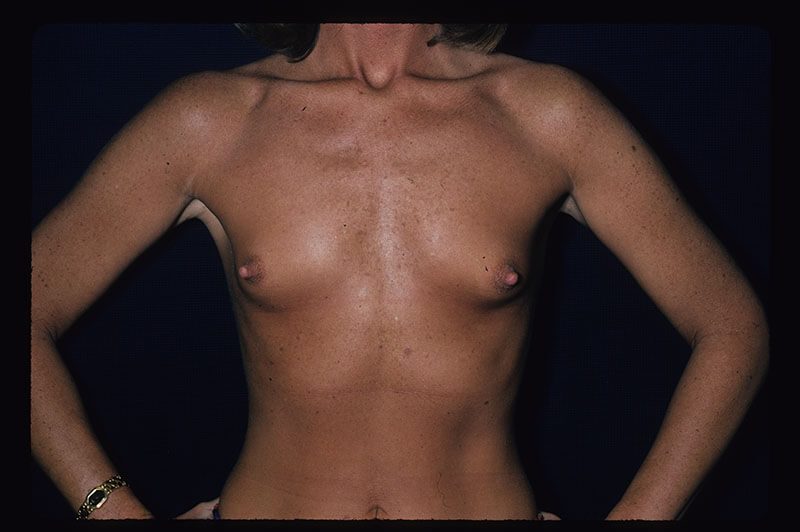
Patient was 36 yr. old, no children, 5’8” 130 lb. 36-AA before initial breast augmentation with subpectoral 450 cc smooth high profile gel implants inserted via axillary (armpit) incisions with endoscopic assistance.
Left side: 2 months after breast augmentation became excessively firm and immobile but moved over chest wall adequately after repeated massage. Patient did not wish further improvement on left for grade III firmness. (note: her operation was before Keller funnel became routinely used to minimize chance of contamination and contracture after axillary gel augmentation)
Right side: continued to settle too low i.e. “bottom out” despite efforts to slow its descent.
Operation: Right side only six months after breast augmentation original operation. Patients own capsule tissues used to raise fold under right breast. Capsulo-capsulorrhaphy via infra mammary incision. Implant removed. Absorbable sutures are placed inside the pocket and checked from the outside to be sure fold at the proper level with pleasing smooth curvature. Any dimples are marked and the sutures removed/placed, adjusted until with sizer implant perfectly smooth pleasing shape and position achieved. Dr Pertsch uses his hand on the upper breast to mimic the effect of upright posture/ gravity to best assure symmetry after surgery. The temporary internal sutures were then reinforced with a permanent woven suture internally. The patients upper capsule had also been internally released so the implant could temporarily slide higher and not put pressure on the capsulo-capsulorrhaphy repair A final check with the sizer implant was followed by placing the original 450 cc gel high profile implant. After surgery she wore one of her own brassieres modified by Dr. Pertsch to be cupless with padded underwire support of the repair for 6 weeks.
Her original axillary incision did not provide enough access to perform a capsulo-capsulorrhaphy thus the need for another incision on the undersurface of her right breast to accomplish the surgery.
The patient’s tissues seemed adequate enough without the need for Strattice ACD to reinforce the capsule repair.
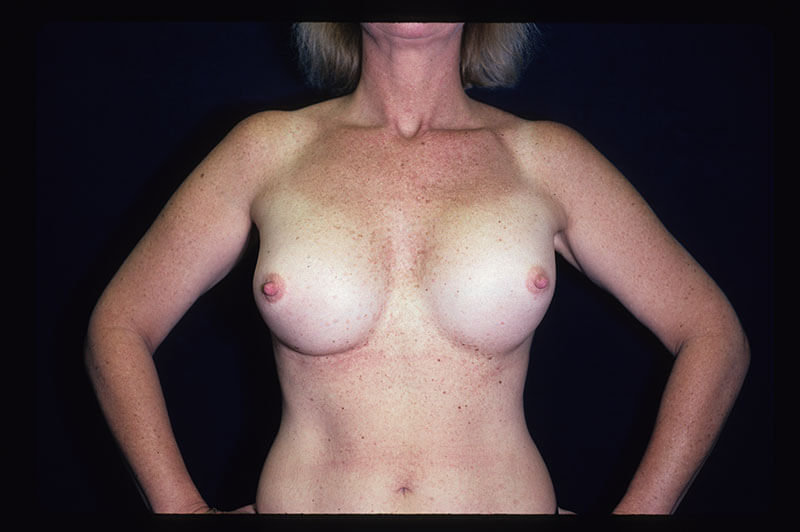
Photographs taken 4 yrs. 9 mo. after repair.
Close up show new infra mammary incision on right side, and original axillary incisions on both sides.
Both breasts had a soft and natural feel. They moved well within their pocket contributing to a natural feel. Still 5’8” 130 lb. when after pictures taken. Happy with her 34D brassiere size. Some 36C fit but others the underwire is a little too wide.
Bottoming Out Patient 02











Description:
Presented to Dr. Pertsch proclaiming she “wants her breasts to look amazing!”
23 y.o. lady had transumbilical subglandular breast augmentation elsewhere 2 yr. 3 mo. prior. Saline implants 510 cc filled to 550 cc o both sides per operative report. The day after surgery right side deflated and required replacement. Her breast implants settle too far below and to the side: “bottomed out”. When she laid down the implants “disappeared off to the side”. Further there was diffuse rippling. She was happy with her 32D size but unhappy otherwise.
Exam 5’5” 110 lb. 32D very slender: almost no subcutaneous fat or breast tissue to cover implants. There was palpable rippling over her entire breast and some visible rippling due to saline subglandular implants. Implants had bottomed out, settled to far below and to the side.
Preoperatively markings were carefully done with measurements to determine best place to place Strattice ACDto provide better implant support. In addition the Strattice will provide more cover over the implant below the muscle to reduce rippling. Patient wanted saline implants again although silicone gel can more reliability reduce rippling.
Dr Pertsch revision surgery:
Via periareolar incision, general anesthesia
Old intact implants removed: These were 510cc minimum fill moderate profile smooth saline. Right side had 586 cc, and left side had 535 cc. (note: this is different than reported in the previous surgeon’s operative report: preoperative preparation provides options for the inevitable surprises with breast implant revision surgeries. Having various size implants available in the OR assured Dr Pertsch’s surprise during surgery does not become an unpleasant size surprise for patient after surgery!)
Implants placed in pocket created under pectoralis major muscle to minimize rippling on upper inner breast.
Existing capsule sutured to the new higher position and tightened on the sides.
Strattice ACD (Acellular dermis) (22 cm x 10cm) used from muscle down to ribs:
- Assured better support for the sizable implant in the new higher position. Less chance of her own thin tissues stretching and bottoming out yet again.
- Adds more tissue to cover the lower part of the implant to minimize rippling,
- Minimizes breast motion (“animation effects”) in the new submuscular location.
New smooth saline high profile implants were filled to maximum 550 cc volume on both sides to minimize rippling.
Photo preop and with preoperative markings.
Photo with patient brassiere modified to be cupless with padded underwire worn for support 6 weeks after surgery
After photos 1 yr. 2 weeks
Image 0020 muscle relaxed, and image 0021 with patient contracting her pectoral muscle shows minimal animation, i.e. minimal motion of breast with muscle/ arm usage after surgery
She wore the cupless underwire brassiere created by Dr.Pertsch modifying one of her own old brassieres as support for breast until internal suture healed 6 weeks after surgery.
There was no visible or palpable rippling after surgery.
Breasts felt soft and moved naturally and did not slide off to the side as they had before surgery.
She was very happy with results.
Bottoming Out Patient 03